I remember going into labor with my first child like it was yesterday. My water broke, and the contractions came fast and quick. I felt overcome with nausea and the pain of contractions as my husband grabbed our overnight bags, called my doula, and drove us to the hospital in a rush. When labor began, and I was pushing our daughter out, I was grateful I knew what medical interventions I might need for pushing. I was also grateful that we had a written birth plan, taken childbirth classes together, and hired a doula who was by my side, advocating on my behalf during labor and delivery. The prior knowledge of medical interventions I might need during delivery made me feel more confident. It also made the whole process of my labor and delivery go smoother.
You may have heard about medical interventions that can occur during labor, such as induction via membrane sweep, Pitocin, or an amniotomy. But do you know what medical interventions you might need during actual pushing? In this article, we’ll explain these in detail and share how you can help lower your risk of needing interventions.
Medical Interventions You May Need During Pushing
I was so glad that I had a doula to explain these medical interventions to me before I delivered my children. Let’s explore them below:
1. Epidural

An epidural is a spinal anesthetic that mothers receive during childbirth to relieve pain.4 Epidurals are the most common type of pain relief used during childbirth in the United States.4,5 They’re usually administered when the cervix is dilated to 4-5 centimeters and given by an anesthesiologist. Intravenous (IV) fluids will be started before an epidural is placed. An obstetrician or nurse anesthetist will administer the epidural through the IV/catheter process.4
I used an epidural with both of my deliveries. I delivered my daughters just fine, my recovery was normal, and both my daughters breastfed beautifully. For the birth of my first child, I had written in my birth plan that I didn’t want an epidural. But I never regretted getting one once my pain reached levels I couldn’t handle without medicine. Each woman is different, however. Making a birth plan with your specific preferences and goals for delivery — and then being okay if they need to change — can be a helpful way to make your birthing process smoother.
2. Episiotomy

Episiotomies in childbirth used to be the norm. However, the past few decades of research have revealed that surgical cuts may not be as beneficial as medical professionals once believed.1 Your healthcare provider will make the episiotomy in the perineum right before the baby’s head comes out. This is the area between the vagina and the rectum.1,5,7 The doctor will stitch up a small cut or incision after delivery.7
Generally, a mother doesn’t need an episiotomy in a healthy birth without any complications. But suppose there are complications during delivery that endanger the mother or baby. In that case, the mother may need an episiotomy to ensure a faster delivery or protect the child’s safety.7
At my request, my obstetrician allowed my perineum to tear naturally during childbirth. Then, she stitched it up afterward. I was glad we did it this way. My perineum healed normally without infection, and the natural tear wasn’t severe.
3. Fetal Monitoring

Fetal monitoring is a technique used to check the baby’s heart rate.8 Auscultation is fetal monitoring done using a stethoscope/fetoscope or Doppler transducer to listen to baby’s heart rate.8,9 This is the same equipment an obstetrician uses during prenatal visits.9 Electronic monitoring records baby’s heart rate via a fetal monitoring Doppler belt placed around the abdomen. Internal monitoring requires an electrode to be placed on the part of the baby closest to the cervix — usually their scalp.8,9 Changes in their heart rate can indicate a problem, such as baby not getting enough oxygen.9 Fetal monitoring can help medical professionals determine if a C-section is necessary.10
I recall having the Doppler bands around my belly both times I gave birth. They didn’t bother me, and I hardly noticed them. I was glad to know my child’s heart rate was being monitored. If a mother is wearing a Doppler band and feels uncomfortable, a nurse can help adjust the band for improved comfort.
4. Forceps
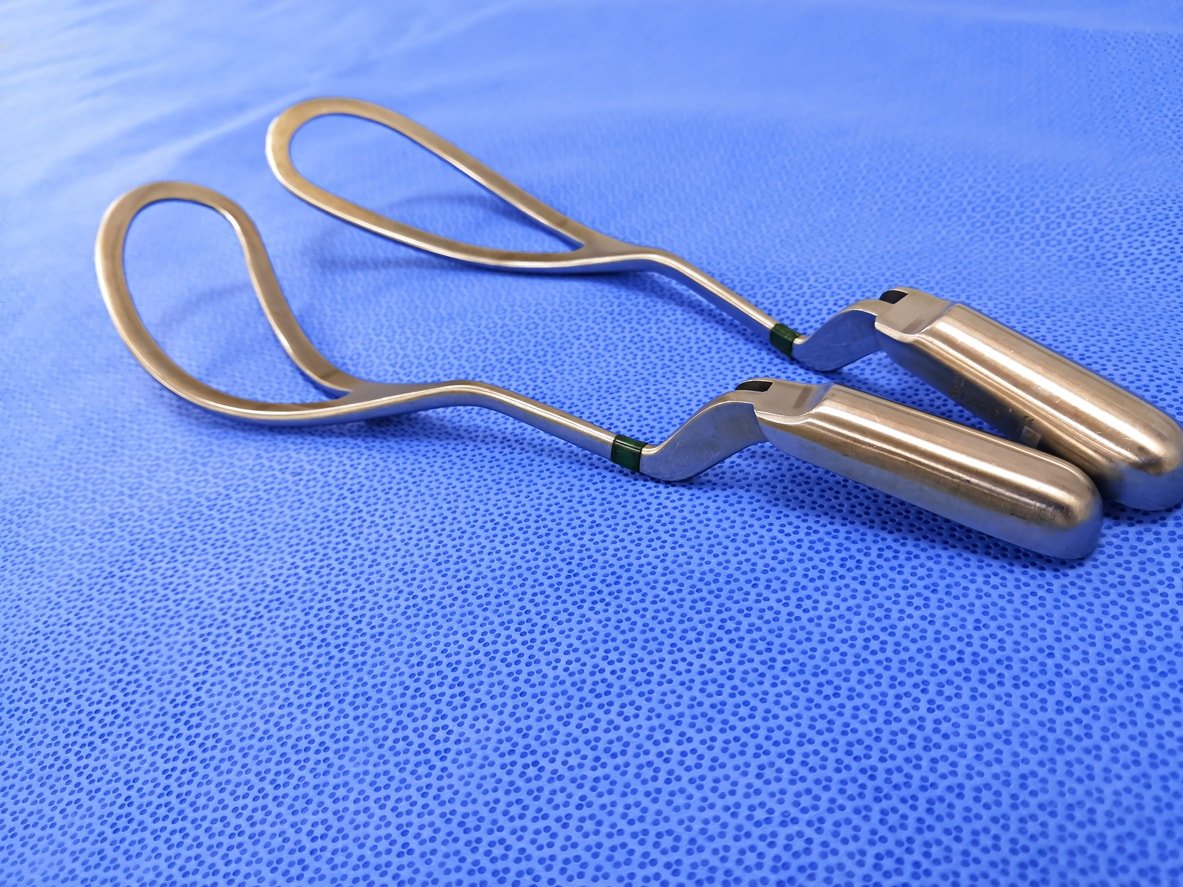
Forceps interventions are rare during delivery and used in only 0.5% percent of vaginal births. A doctor may use them if the mother or baby shows signs of distress and delivery needs to be sped up.11 A forceps delivery occurs once the mother is fully pushing.12 It can be an alternative to having a C-section if there’s fetal distress.11
A mother’s cervix must be fully dilated, and membranes must be ruptured. An episiotomy may be performed, and they’ll anesthetize the area unless an epidural has already been administered.11,13 Between contractions, your obstetrician will insert the forceps into the vaginal canal, placing each forceps on either side of your baby’s head. As you push, the doctor will use the forceps to guide baby out of the birth canal gently, but they’ll only use the forceps for as long as they’re helping.11 Bruising of the baby’s head and (in rare cases) bleeding or facial nerve damage may occur, making forceps a less-than-desirable choice but certainly worthwhile if necessary.12
5. Vacuum Extraction

Like forceps, vacuum extraction is another type of assisted delivery that may be necessary if the baby is distressed and delivery is stalled. For example, your doctor may perform a vacuum extraction if labor is no longer progressing and the baby is stuck in the birth canal.14 Another example is if a mother feels too tired to push, has a heart condition, or has very high blood pressure. The doctor could also do it if baby is experiencing distress, as indicated by a change in heart rate.14,15
In a vacuum procedure, the doctor will place a vacuum extraction cup onto the baby’s head between a mother’s contractions. During the contractions, the doctor will use the vacuum pump to create suction to move baby through the birth canal and prevent baby’s head from moving back up between contractions. The doctor can remove the suction cup once baby’s head comes through. The mother can push the rest of baby’s body out.12,16 Vacuum procedures are more common than forceps delivery.2 But it’s likely that an obstetrician will go with a C-section instead of vacuum extraction if the delivery process has stalled.14
6. C-Section

A cesarean section, or C-section, is a surgical procedure to deliver a baby through an incision in a mother’s abdomen. This is an option if a mother has been pushing but the vaginal delivery is not progressing.6 Examples of transitioning from a vaginal delivery to an emergency C-section include:6,17
- Problems with the umbilical cord wrapped around the baby
- A change in the baby’s heart rate, causing distress
- Concerns for the mother’s health
- A twin or multiples delivery
- Other medical emergencies
According to the Mayo Clinic, this procedure requires anesthesia to numb the lower half of the mother’s body (such as regional anesthesia), allowing the mother to remain awake during surgery. Some of the typical choices for numbing the pain include a spinal block or epidural block. Sometimes, you need general anesthesia for an emergency C-section.6 While it typically takes longer to heal from a C-section than a vaginal birth, it can be a life-saving measure.18
How To Avoid Interventions During Pushing
It’s impossible to be sure that you won’t need medical interventions during pushing, but there are ways to lower your risk. And don’t worry if you do need medical intervention — childbirth is about the process, not perfection! Here are a few tips to help you potentially avoid interventions:
1. Write a Birth Plan
Taking the time to write out your birth plan will give you prior knowledge about what to expect. It will also help you clarify what you want to occur during your labor and delivery. Writing a plan isn’t about ensuring it will go exactly as planned down to the last detail. Instead, you aim to get most of your goals down on paper and then share them with the medical professionals performing the delivery. Many moms report that having a birth plan gave them confidence and authority over their labor and delivery.19 This kind of positive visioning may assist in making the birthing process go more smoothly.20,21
2. Take a Childbirth Course

Enrolling in classes during pregnancy, like a childbirth class, can help the mother and her partner or delivery companion learn what to expect. The more knowledge a mother possesses, the better she can make choices or ask for what she needs during labor and delivery. This is also helpful for those assisting in her delivery, such as family members.
3. Work With a Midwife or Doula

A midwife usually works at a birthing center or the mother’s home for the delivery. Their care and expertise may reduce a woman’s risk for medical interventions.3 A doula is a childbirth advocate who can help you write your birth plan, meet with you before and after your delivery, and be present in the delivery room if you choose to have your baby at a hospital.22
Read our full article about the differences between a doula and a midwife and why you might want to hire both.
Some of these medical interventions are more common than others. By having a better understanding of each, we hope that you feel more prepared and confident for your birthing day!