After nine long and tiring months, you’re more than ready for your bundle of joy to make its way into the world. You’ve anxiously waited for the moment when your water breaks and you have to rush to the hospital. You’ve even dreamed of holding your little one for the first time. But before you can examine your baby’s precious face for your eyes and your partner’s smile, you have to get through labor first. As with everything in a pregnancy, there’s always room for unpredictability. You may need to medically induce labor with the help of your provider and one of these labor induction methods.
When Will a Doctor or Midwife Recommend an Induction?
There are some conditions when a doctor or midwife recommends a medical induction. First, they’ll evaluate your and your baby’s health. They’ll consider your baby’s gestational age, the weight and size of your baby, your baby’s position in the uterus, and the status of your cervix.1,3 After weighing the benefits and risks, you and your care provider will determine if a medical induction is the next best step. According to the Mayo Clinic, these are the medical reasons for an induction:1
- Post-term pregnancy: You’re approaching two weeks beyond your due date, and labor hasn’t started naturally.1
- Prelabor rupture of membranes: Your water has broken, but you aren’t having any contractions.1,3
- Chorioamnionitis: Your uterus has an infection.3 (This is why your medical team will routinely check your temperature to ensure it isn’t elevated, which can be a sign of an infection.6)
- Fetal growth restriction, or intrauterine growth restriction (IUGR): The baby doesn’t grow at the expected rate during the mother’s pregnancy, and the estimated weight of the baby is less than the 10th percentile for gestational age.1,4
- Oligohydramnios: This is when there’s a low amount of amniotic fluid around the baby.1,3
- Gestational diabetes: This is when you develop diabetes during pregnancy.1,3
- High blood pressure disorders of pregnancy: These include:1
- Preeclampsia: This is a pregnancy complication characterized by high blood pressure and signs of damage to another organ system, commonly the liver and kidneys. It usually begins after 20 weeks of pregnancy in women whose blood pressure has been normal.3,6
- Chronic high blood pressure: This refers to high blood pressure that was present before pregnancy or occurred before 20 weeks of pregnancy.5
- Gestational hypertension: Gestational hypertension is high blood pressure that develops after 20 weeks of pregnancy.6
- Placental abruption: This is when the placenta detaches from the inner wall of the uterus before delivery — either partially or entirely.1
- Certain medical conditions: Other medical conditions, such as kidney disease, can be a reason for labor induction.1
Different Labor Induction Methods
Here’s what you need to know about the available induction methods that a doctor or midwife may recommend to get your body in labor mode:
1. Amniotomy
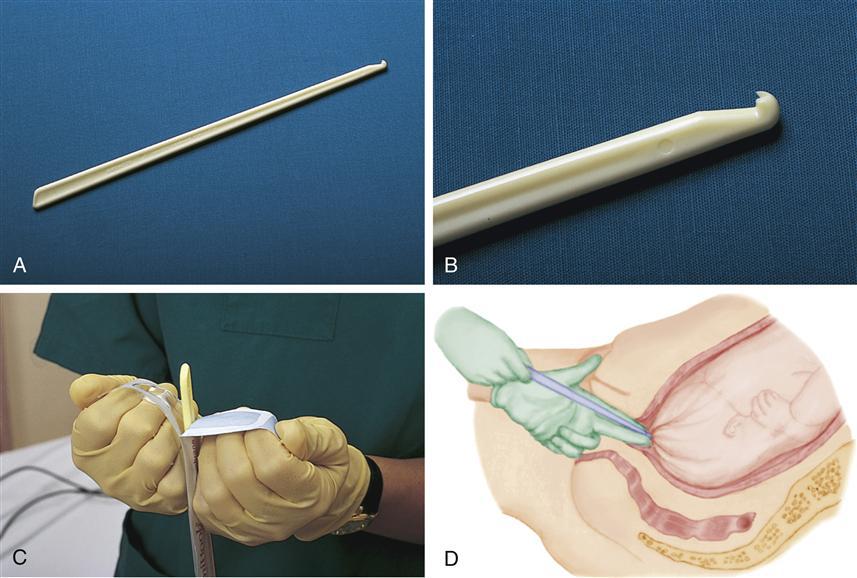
An amniotomy is a procedure in which your doctor will deliberately rupture the amniotic sac. This is also referred to as artificial rupture of membranes (AROM), or most popularly, “breaking the water.”7 They complete this process while you’re in bed in the labor and delivery room.7 Your provider will insert a small surgical hook (called an amnihook) into the vagina and through the cervix to puncture the membranes within the amniotic sac.3,7 This will release the amniotic fluid and natural hormones that can stimulate contractions.7,8 There aren’t any nerve endings in the amniotic sac, so this is a painless procedure.3,9 It feels like a cervical exam and then a release of warm fluid.10 Once the procedure is over, moms-to-be typically go into labor within a few hours (but this isn’t guaranteed).11,12
2. Cervidil (Dinoprostone)

For pregnant mommas who are at or near the end of their pregnancy, Cervidil is an option that physicians may recommend to help ripen (aka soften) and dilate the cervix.2 The vaginal insert is infused with a synthetic version of prostaglandin — a hormone-like substance naturally occurring in the body and responsible for the cramps you feel during your period.2,13 Through the use of prostaglandins, the muscles of the cervix relax, and labor can begin.2,14
Your healthcare provider inserts Cervidil (which is similar in shape and size to a tampon) into the vagina. It will remain in place until you no longer need it or after 12 hours.2,14 You’ll notice a long tape attached to the insert, but it’s important not to tug on or remove it, as it’s necessary for when your doctor has to take it out.15 (Here’s a video to see how they administer it.)
3. Cytotec

Cytotec is for pregnant women whose cervix is long, closed, or unripened.16 It helps soften the cervix so it can properly dilate and produce uterine contractions.16,17 Cytotec is provided in pill form and ingested orally with water. Another option is to have the pill inserted into the end of your vaginal canal (called a vaginal Cytotec).16 The pill will dissolve quickly and is longer-acting than the oral form.18
4. Foley Balloon
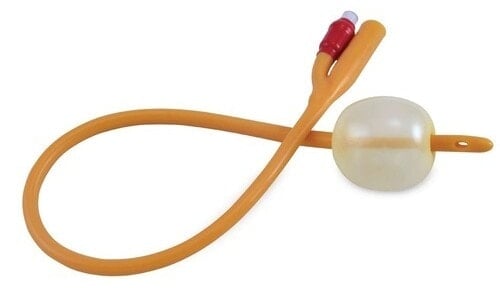
A foley balloon (or Foley bulb) is a small, balloon-like instrument attached to the end of a catheter.19 It’s used to open the cervix and help it reach effacement (the cervix is stretched and becomes thinner).19,20 The uninflated balloon is inserted into the cervix through the catheter and filled with saline solution to inflate the device. The Foley bulb will apply pressure to the cervix to help dilate it. Once the cervix has dilated (usually about 3-5 centimeters), the Foley balloon will fall out.19
5. Membrane Stripping/Sweeping
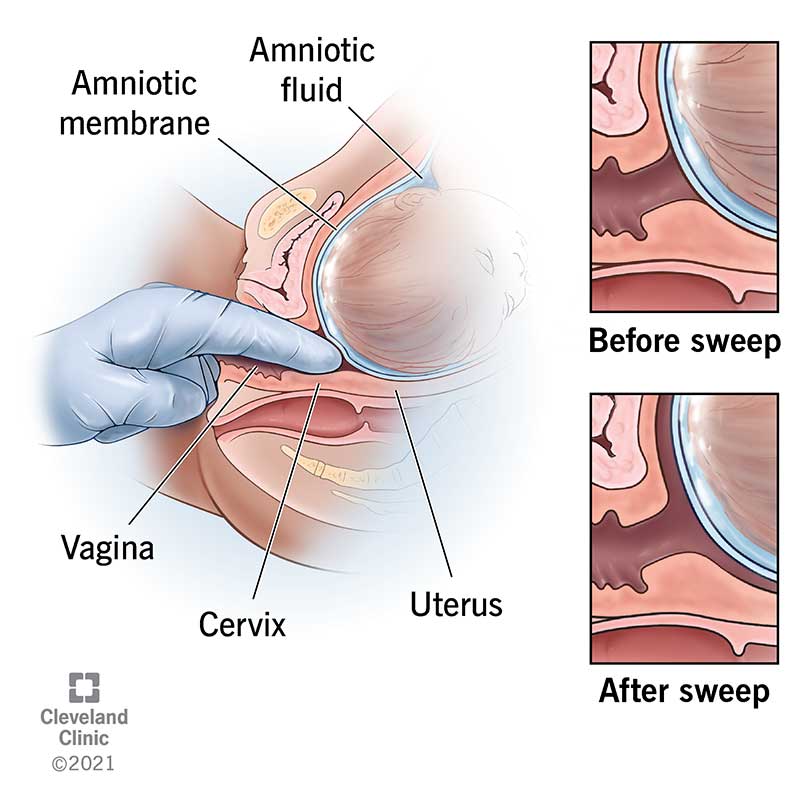
Membrane stripping, or membrane sweeping, is a procedure that your doctor completes when you’re either full term (39 to 41 weeks of gestation) or partially dilated to help induce labor.3,21 You can complete membrane sweeping during your regular physician visit when you’re close to or past your due date.21 Your doctor will insert a finger into the vagina and up through the cervix to manually move and separate the thin membranes connected to the amniotic sac.1,3,11 When the membranes are stripped, the body can release prostaglandins to help produce contractions and prep the cervix for delivery.3,11
6. Pitocin

To help kick-start contractions, your physician may recommend the use of Pitocin.3 This is one of the most common labor induction methods. The medication, a commonly used drug in labor, is the artificial variation of oxytocin.1,3,22 Oxytocin is a natural hormone produced to help the uterus contract and is released when a woman’s body is ready for childbirth.1,3,23 Your provider will administer Pitocin intravenously in your arm while you’re in the labor and delivery suite.3,16 The nurse will slowly increase the dosage to start your contractions.16 They remove it when you’re experiencing contractions that are two to three minutes apart.16,24
Whether your body can induce labor naturally or you need one of these labor induction methods, all that matters is being able to hold your new baby in your arms. But knowing your options before you begin the process will help you and your provider make the best choice when and if needed.